
Breast Cancer
building on our history and evolving with the science
Home / Our therapy areas / Oncology / Breast Cancer
At AstraZeneca our aim is to help improve the outcomes of breast cancer patients with the ambition to one day eliminate cancer as a cause of death. Throughout our history, our innovative science has led to potential practice-changing medicines for patients with breast cancer, and although we have come so far, there is still much to be done. We are committed to furthering our research to redefine the breast cancer treatment paradigm.
Breast cancer remains the most common cancer in women around the world1 and is the leading cause of cancer death in women.2 Men are susceptible to breast cancer, although at a far lower rate than women.3 It can begin in various parts of the organ, including the ducts, the lobules (which make milk), or the tissue in between.4
Breast cancer care has transformed over the last 50 years5, and we’re proud to have continuously supported this through research.
The introduction of mastectomy (a surgery to remove the entire breast6) and chemotherapy into clinical practice, as well as advancements in screening and diagnosis, namely mammography, and increased disease awareness have significantly improved the survival of people living with breast cancer.4,7
With progress in molecular biology, systems biology and genome sciences in recent years, we have expanded our understanding of breast cancer at the cellular, molecular and genomic levels.4 We know now breast cancer is one of the most biologically diverse tumour types with various factors fuelling its development and progression.4
Today we can classify and help to treat those living with breast cancer by their hormone receptor or HER2 expression status, as well as whether they have a BRCA mutation. But as our understanding of the different factors fuelling breast cancer grows, so will our ability to develop potential medicines for new subtypes of patients.
How we classify breast cancer today
To help determine the best management approach for breast cancer, it is critical to identify key receptors or proteins that may be driving the tumour growth. The expression of receptors or proteins in turn determines how the breast cancer is classified.

Breast cancer classification – hormone receptors
Hormones are the driving factor in the development of breast tissue, so it’s no surprise they also play a critical role in the development of cancerous tissue in the breasts as well - in fact, their role in tumour formation has been well documented for over a century.8 The growth and proliferation of female breast tissue occurs during puberty when hormonal stimulation triggers cellular differentiation. The changes in puberty are heavily influenced by the steroid hormones, oestrogen8 and progesterone, which act as the ‘master regulators’ of the development of regular functions of the breasts.9
The two steroid hormones bind to cellular receptors and stimulate growth. Unfortunately, this exact mechanism is exploited by tumour cells which also use oestrogen and progesterone to fuel their growth.10
The presence of oestrogen receptors (ER) and/or progesterone receptors (PR) on tumour cells is used as one of the main classification methods of breast cancer. To be labelled as hormone receptor (HR)-positive, over 1% of breast cancer cells must express ER, or both.11 The cancer is labelled as hormone receptor (HR)-negative when less than 1% possess these receptors11 (if any receptors at all) and it is unlikely the cause of tumour growth.12
The role of hormones in breast cancer has been well understood for some time, and as a result some of the first medicines designed specifically for breast cancer were hormone therapies.10 These therapies prevent the cancer cells from using oestrogen or progesterone and can work in various ways.
Oestrogen receptors are far more prevalent than progesterone receptors in breast cancer, with approximately 80% of all breast cancers being hormone-dependent and oestrogen receptor-positive (ER+).13 Cases of tumours being oestrogen receptor-negative/progesterone receptor-positive (ER-/PR+) are extremely rare14 and, therefore, treatments often target pathways involving oestrogen – these are often called endocrine inhibitors.15
The role in guiding treatment opinions: Aromatase inhibitors (AIs), for example, prevent oestrogen from being produced by certain tissues (other than the ovaries), while other therapies known as selective oestrogen receptor modulators (SERMs) compete with oestrogen to bind to receptor, thereby blocking the effects of oestrogen.15
Another method of targeting HR+ breast cancer is to selectively degrade the oestrogen receptor with the use of selective oestrogen receptor degraders (SERDs).16 By degrading the oestrogen receptor, the ER signalling pathway is broken and the cancer cells ability to use oestrogen is snatched away. SERDs are often used in metastatic disease17 - where the cancer has spread to other parts of the body - and are increasingly used in combinations with other agents to potentially overcome resistance to endocrine therapies.18,19
The number of medicines available for HR+ breast cancer has continued to grow in the past few decades, but there is still more to be done. Now we are striving to further transform the lives of women with HR+ disease by building on our rich heritage.
Breast cancer classification – HER2 receptors
In the early 1980s, the human epidermal growth factor 2 (HER2) gene, which helps maintain a healthy cell lifecycle, was found to fuel excessive cancer cell growth and proliferation in breast cancer cells when there is overexpression of the HER2 gene or protein.20
High levels of HER2 protein expression is found in approximately 20% of breast cancers and is associated with aggressive and fast-growing disease.13
{kind=link}
The role in guiding treatment options: Although traditionally HER2+ breast cancer is associated with poor prognosis21, this has improved meaningfully as monoclonal anti-HER2 antibodies, tyrosine kinase inhibitors and antibody-drug conjugates (ADCs) have been developed to target the oncogenic driver.22
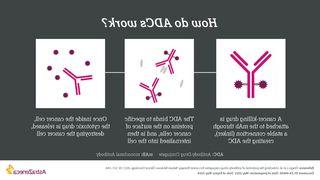
ADCs consist of two cancer-fighting medicines in one, a cytotoxic agent, also known as chemotherapy or the “payload”, and a monoclonal antibody (that binds to a specific target expressed on cancer cells) joined together by a linker. This enables the highly targeted delivery of a cytotoxic agent, which is known for having poor specificity towards cancer cells, directly into the cancer cell thereby potentially sparing normal cells.23 To learn more about ADCs, click here.
Breast cancer classification – Triple-Negative Breast Cancer (TNBC)
Triple-negative breast cancers (TNBC) do not express oestrogen receptors, progesterone receptors and do not have high levels of HER2 overexpression, so they are considered ‘negative’ for all three. TNBC accounts for 10-15% of all breast cancers and is more common in women under 40. This specific form of breast cancer is known to be particularly aggressive and fast growing, with a high risk of metastasis and, unfortunately, is more likely to recur after treatment than other breast cancers.24,25
The role in guiding treatment options: The number of treatment options available for TNBC is significantly less than that of other forms of breast cancer due to the lack of known actionable biomarker targets. As with most breast cancers, if the disease has not yet metastasised, surgery is usually employed with chemotherapy used to either shrink the tumour before surgery or reduce the chance of the cancer coming back following surgery. In some circumstances, women with TNBC may also be eligible for immunotherapy where the body’s own immune system is harnessed to fight the cancer.24
Breast cancer classification – BRCA mutations
Developments within genomics identified further biomarkers which can be actioned to target breast cancer, specifically, the two BReast CAncer susceptibility (BRCA) genes – BRCA1 and BRCA2.26
The two BRCA genes are considered ‘tumour suppressors’ and repair damage caused to our DNA in a process known as the DNA Damage Response (DDR), specifically in homologous recombination repair (HRR), which is just one of the pathways to do so. It’s worth noting that also part of DDR, a family of enzymes known as PARPs (Poly(ADP-Ribose) Polymerases) helps to repair damage through another pathway.27
When the BRCA genes are mutated, they cannot perform their function and the risk of developing cancer increases.28 On average, a woman with a BRCA1 or BRCA2 gene mutation has up to a 7 in 10 chance of acquiring breast cancer by age 80.29
The role in guiding treatment options: At a cellular level, mutated BRCA genes lead to dysfunctional HRR pathways and to survive, the cell must rely on other pathways. This is what can be exploited through targeted therapy. PARP inhibitors trap the PARP enzyme and prevent single-stranded DNA breaks from being repaired. This leads to increases in double-stranded DNA breaks, which cannot be repaired by the dysfunctional HRR pathway. The cell, then must rely on a back-up pathway that is less accurate and prone to error at which point the level of DNA damage goes beyond the manageable limit and leads to cancer cell death.30
AstraZeneca is committed to investigating the potential of DDR inhibition in breast cancer. To learn more about DDR, including other molecules involved and how inhibition of DDR pathways can results in a targeted treatment approach, click here.
How will we transform the way we classify and treat breast cancer in the future
To truly succeed in reaching our goal of eliminating cancer as a cause of death we must change the practice of medicine.
For over 40 years, AstraZeneca has contributed to advancements in breast cancer care, with a series of pioneering medicines, including targeted monotherapies and precision/personalised combinations, which continue to have a critical role in improving outcomes for women with breast cancer.
Breast cancer remains a focus for AstraZeneca. As our understanding of the features that fuel this complex tumour type grows, the way we classify breast cancer and the way we treat will undoubtedly change, something we are spearheading at AstraZeneca. We are leading an exciting phase of scientific discovery and innovation and are identifying novel ways of improving outcomes for patient populations which are associated with poor clinical outcomes. We continue to strive for improved testing to identify the actionable targets of an individual’s breast cancer and bring the benefits of a biomarker-driven approach to even more patients
To help address the ongoing unmet medical needs, we are exploring different mechanisms of action that address the biologically diverse breast cancer tumour environment at every stage of the disease continuum and across the various lines of treatment. Utilising our ever-growing understanding of the underlying breast cancer biology, we are dedicated to redefining treatment pathways and to help transform the lives of those living with breast cancer.
References
- Siegel R, et al. Cancer statistics, 2020. A Cancer Journal for Clinicians. 70(1), pp.7-30.
- World Health Organization. IARC. Estimated number of deaths in 2018, worldwide, females, all ages. Available at http://gco.iarc.fr/today/online-analysis-table?v=2018&mode=cancer&mode_population=continents&population=900&populations=900&key=asr&sex=2&cancer=39&type=1&statistic=1&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17&group_cancer=0&include_nmsc=1&include_nmsc_other=1 Accessed May 2022.
- Gucalp A, et al. Male breast cancer: a disease distinct from female breast cancer. Breast Cancer Res Treat. 2019;173(1):37-48.
- Feng Y, et al. Breast cancer development and progression: Risk factors, cancer stem cells, signalling pathways, genomics, and molecular pathogenesis. Genes & diseases. 2018;5(2), 77–106.
- Cancer Research UK. Cancer in the UK 2019. Available at http://www.cancerresearchuk.org/sites/default/files/state_of_the_nation_april_2019.pdf Accessed May 2022.
- Cancer.org. Mastectomy | Mastectomies For Breast Cancer. Available at http://www.cancer.org/cancer/breast-cancer/treatment/surgery-for-breast-cancer/mastectomy.html Accessed May 2022.
- World Health Organisation. WHO position paper on mammography screening. Available at http://apps.who.int/iris/bitstream/handle/10665/137339/9789241507936_eng.pdf;jsessionid=6ABDEA86654F84E089CCEF024C8E2009?sequence=1 Accessed May 2022.
- Trabert B, et al. Progesterone and Breast Cancer. Endocr Rev. 2020;41(2):320-344.
- Hilton H, et al. Estrogen and progesterone signalling in the normal breast and its implications for cancer Development. Molecular and Cellular Endocrinology. 2018;466, pp.2-14.
- Cancer.Net. Estrogen And Progesterone Receptor Testing For Breast Cancer. Available at http://www.cancer.net/research-and-advocacy/asco-care-and-treatment-recommendations-patients/estrogen-and-progesterone-receptor-testing-breast-cancer Accessed May 2022.
- Allison K, et al. Estrogen and Progesterone Receptor Testingin Breast Cancer. American Society of Clinical Oncology/College of American Pathologists Guideline Update. Arch Pathol Lab Med. 2020;144:545-563.
- Cancer.org. Breast Cancer Hormone Receptor Status | Estrogen Receptor. Available at http://www.cancer.org/cancer/breast-cancer/understanding-a-breast-cancer-diagnosis/breast-cancer-hormone-receptor-status.html. Accessed May 2022.
- WebMD. Types of Breast Cancer. Available at http://www.webmd.com/breast-cancer/breast-cancer-types-er-positive-her2-positive#:~:text=About%2080%25%20of%20all%20breast,response%20to%20another%20hormone%2C%20progesterone. Accessed May 2022.
- Arena et al. ER−/PR+/HER2− breast cancer type shows the highest proliferative activity among all other combined phenotypes and is more common in young patients: Experience with 6643 breast cancer cases. The Breast Journal. 2019;25(3), pp.381-385.
- Cancer.org. Hormone Therapy For Breast Cancer. Available at http://www.cancer.org/cancer/breast-cancer/treatment/hormone-therapy-for-breast-cancer.html Accessed May 2022.
- Wang L, et al. New Class of Selective Estrogen Receptor Degraders (SERDs): Expanding the Toolbox of PROTAC Degrons. ACS Medicinal Chemistry Letters. 2018;9(8), pp.803-808.
- Patel H, et al. Selective estrogen receptor modulators (SERMs) and selective estrogen receptor degraders (SERDs) in cancer treatment. Pharmacology & Therapeutics. 2018;186:1-24.
- Rani A, et al. Endocrine Resistance in Hormone Receptor Positive Breast Cancer–From Mechanism to Therapy. Frontiers in Endocrinology. 2019;10.
- Lu et al. Design and Synthesis of Basic Selective Estrogen Receptor Degraders for Endocrine Therapy Resistant Breast Cancer. Journal of Medical Chemistry. 2019;62, pp.11301-11323.
- National Cancer Institute. HER2 Genetic Link To Breast Cancer Spurs Development of New Treatments. Available at http://www.cancer.gov/research/progress/discovery/her2 Accessed May 2022.
- Wang J, et al. Targeted therapeutic options and future perspectives for HER2-positive breast cancer. Signal Transduction and Targeted Therapy. 2019;4(34):1-22.
- Rinnerthaler G, et al. HER2 Directed Antibody-Drug-Conjugates beyond T-DM1 in Breast Cancer. International journal of molecular sciences. 2019;20(5):1115.
- Dan N, et al. Antibody-Drug Conjugates for Cancer Therapy: Chemistry to Clinical Implications. Pharmaceuticals (Basel, Switzerland). 2018;11(2), 32.
- Cancer.org. Triple-Negative Breast Cancer | Details, Diagnosis, And Signs. Available at http://www.cancer.org/cancer/breast-cancer/understanding-a-breast-cancer-diagnosis/types-of-breast-cancer/triple-negative.html. Accessed May 2022.
- Waks A, et al. Breast Cancer Treatment: A Review. JAMA. 2019 ;321(3), pp.288-300.
- Tung NM, et al. BRCA1/2 testing: therapeutic implications for breast cancer Management. British Journal of Cancer. 2018;119:141-152.
- Bohen S, et al. DNA Damage Response –An Emerging Target for Groundbreaking Cancer Therapies. European Oncology & Haematology 2018;14(Suppl 1):2-7.
- National Cancer Institute. BRCA Mutations: Cancer Risk And Genetic Testing. Available at http://www.cancer.gov/about-cancer/causes-prevention/genetics/brca-fact-sheet. Accessed May 2022.
- American Cancer Society. Breast Cancer Risk Factors You Cannot Change. Available at http://www.cancer.org/cancer/breast-cancer/risk-and-prevention/breast-cancer-risk-factors-you-cannot-change.html Accessed May 2022.
- Bonadio R, et al. Homologous recombination deficiency in ovarian cancer: a review of its epidemiology and management. Clinics. 2018;73(Suppl 1).